

Consumer Insights
Uncover trends and behaviors shaping consumer choices today
Procurement Insights
Optimize your sourcing strategy with key market data
Industry Stats
Stay ahead with the latest trends and market analysis.

The global congenital hyperinsulinism treatment market size attained a value of USD 168.32 Million in 2025. The market is expected to grow at a CAGR of 4.80% during the forecast period 2026-2035 to reach a value of about USD 269.00 Million by 2035. The market growth is driven by the increasing awareness of congenital hyperinsulinism and robust pipeline activity globally.
Base Year
Historical Period
Forecast Period
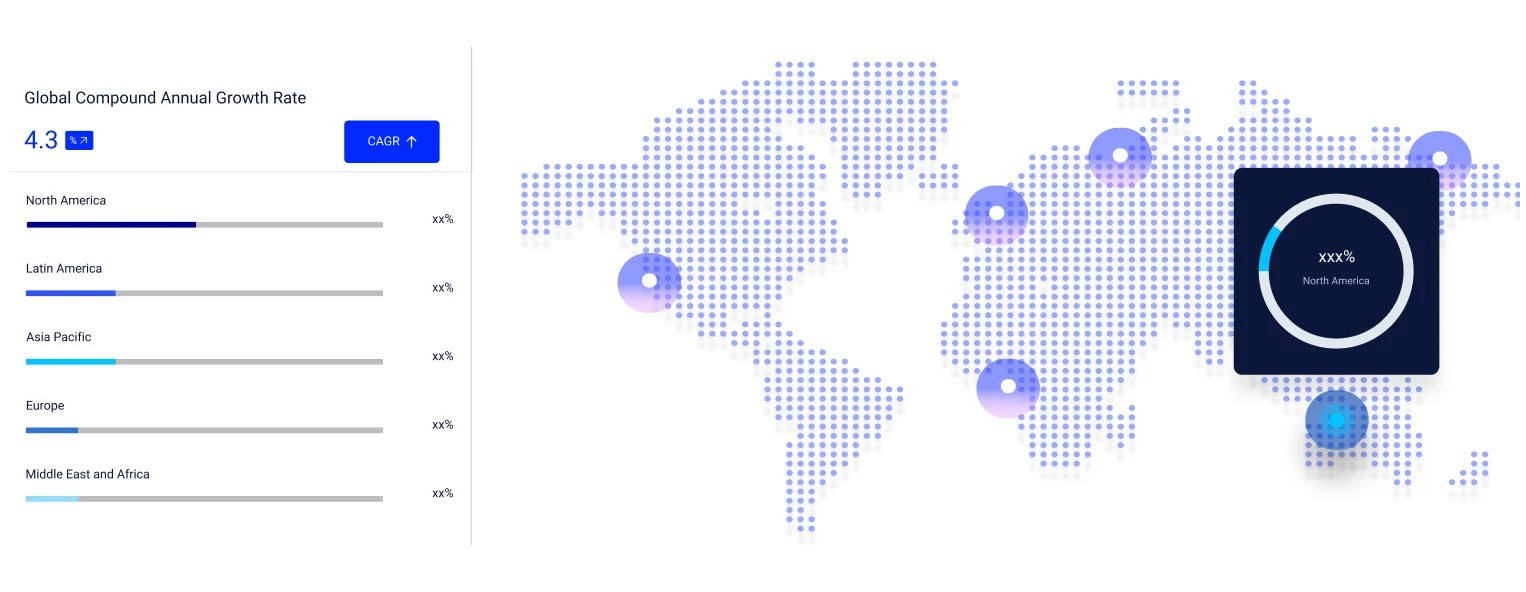
Compound Annual Growth Rate
4.8%
Value in USD Million
2026-2035
*this image is indicative*
Congenital hyperinsulinism treatment market (HI) is a genetic condition in which the pancreatic insulin cells, known as beta cells, secrete an abnormally large amount of insulin. Excess insulin causes low blood sugar or low plasma sugar.
Low blood sugar is extremely harmful since the brain requires a steady supply of sugar. If the brain does not obtain enough sugar, it can cause seizures, brain damage, and even death.
Congenital hyperinsulinism is caused by genetic abnormalities that produce incorrect and excessive insulin release from pancreatic beta cells.
The symptoms of hypoglycemia in infants are frequently difficult to distinguish since it can mimic normal infant behaviours. A few common symptoms include irritability, drowsiness, fatigue, increased food cravings, and rapid heart rate. Whereas moderate to severe symptoms include seizures and coma due to prolonged or extremely low plasma sugar.
Congenital hyperinsulinism is diagnosed using a combination of patient history, laboratory tests, and genetic tests.
The child's history is a vital element of the diagnosis. This includes information such as when the low plasma sugars began, whether the baby was born big for gestational age (LGA), and any family history of low plasma sugars or unexplained newborn deaths, seizures.
Blood tests are required to diagnose HI when the plasma sugar level is less than 50 mg/dL. With a plasma sugar of 50, it will find suppressed ketones and free fatty acids, an elevated insulin level (which may or may not be caught), and a glycemic response to glucagon, with the plasma sugar rising more than 30 mg/dL when glucagon is injected.
To screen for the mutations that cause the most prevalent kinds of HI, DNA from a blood sample from the infant with congenital HI and each parent can be studied. This should be considered for anyone suspected of having congenital HI.
According to the global congenital hyperinsulinism treatment market research report, the market can be categorised into the following segments:
Market Break Up by Diagnosis Method
Market Break Up by Treatment Method
Market Break Up by Treatment Channel
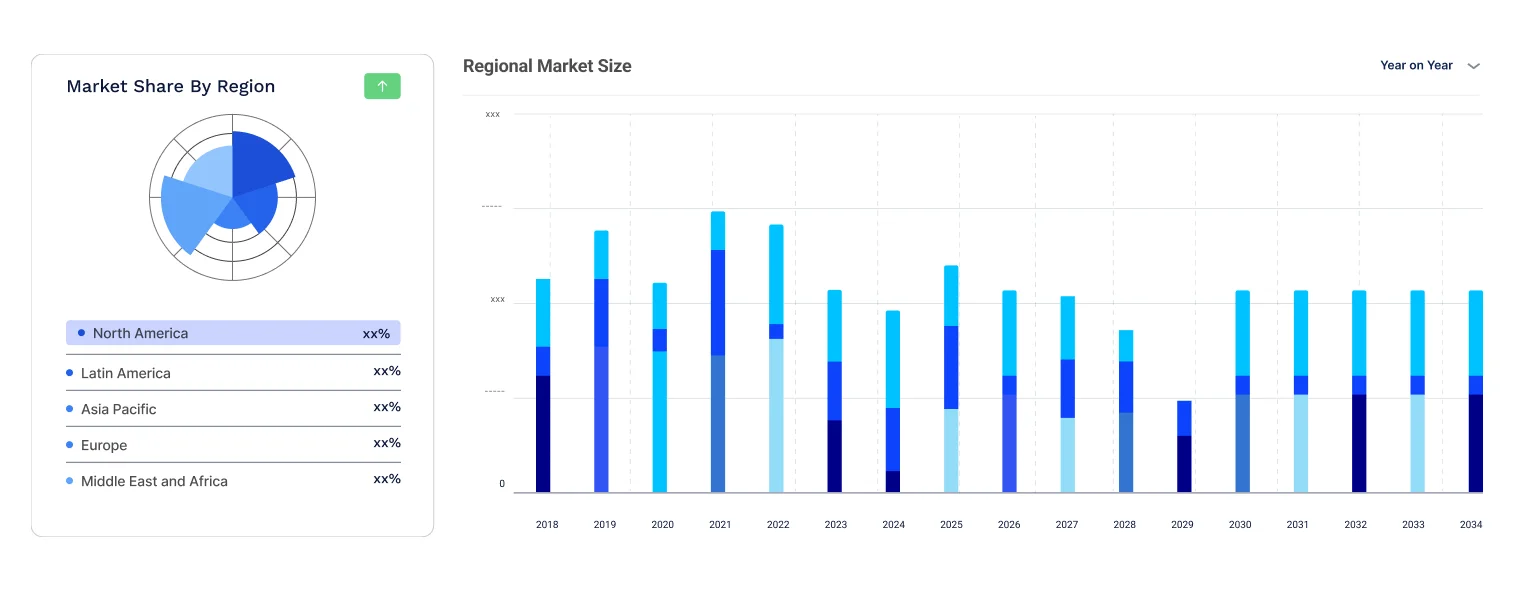
Market Break Up by Region
1 in every 50,000 neonates is born with congenital hyperinsulinism. This disorder is more prevalent in certain groups, affecting up to 1 in every 2,500 births. Approximately 60% of babies with HI are diagnosed within the first month of life. An additional 30% will be diagnosed later in the first year, with the remaining being diagnosed later.
To avoid brain damage, hypoglycemia caused by HI must be treated as soon as possible. Unlike other hypoglycemia-causing situations in which alternate fuels, such as ketones or lactate, may be accessible for the brain during hypoglycemia, HI blocks the generation of these fuels, leaving the brain without an energy source.
Diazoxide, octreotide, and glucagon are among the common medications used to treat HI.
Diazoxide inhibits insulin secretion by acting on the KATP (ATP- Sensitive Potassium Channels) channel. It is often beneficial for newborns with stress-induced hyperinsulinism, GDH-HI (Glutamate dehydrogenase), or GK-HI (Glucokinase), and a subset of children whose underlying problem is unknown. Diazoxide is frequently ineffective in children with KATP-HI.
Octreotide is a medication that decreases insulin secretion as well. Octreotide is frequently quite successful at first, but it may lose effectiveness with time. In neonates, who are already at risk for NEC (necrotizing enterocolitis), octreotide is not currently indicated. Other medicines that are similar to octreotide include octreotide LAR and lanreotide, which have a longer duration of action and can be administered once a month. Longer-acting octreotide preparations are designated for patients who have responded to short-acting octreotide and are on a stable regimen.
Glucagon causes the liver to release glucose. When an infant with HI has low blood glucose levels and cannot be fed, glucagon can be given in an emergency. It works best as a holding therapy while the patient is being readied for surgery.
Children with diffuse KATP-HI frequently necessitate 95-99% pancreatectomies. These procedures are not curative, and KATP-HI children who have had them may still need regular meals and drugs to prevent hypoglycemia. Patient may also require additional procedures. The goal of such surgery is to reduce the intensive medical regimen that would otherwise be required to safeguard young patients from recurring, severe hypoglycemia.
NN414 appears to be a promising replacement for the currently utilised KATP channel opener diazoxide. Targeting KCa3.1 channels with channel openers or L-type Ca2+ channels with DXM or simvastatin may be useful for treating CHI caused by KATP channel mutations that are not susceptible to KATP channel openers.
Exendin-(9-39), an experimental glucagon-like peptide-1 (GLP-1) antagonist, protects fasting and protein-induced hypoglycemia in children with congenital hyperinsulinism. Could possibly be used in the treatment of CHI in children.
The global congenital hyperinsulinism treatment market is expected to propel in the forecast period owing to the robust pipeline activities and increasing awareness of the disease. And the availability of effective therapies will also contribute to driving the market in the future.
The report gives an in-depth analysis of the key players involved in the global congenital hyperinsulinism treatment market, sponsors manufacturing the drugs, and putting them through trials to get FDA approvals. The companies included in the market are as follows:





Upto 15% Off
USD
$3299 $2969
$5499 $4949
$6999 $5949
$8199 $6969






*While we strive to always give you current and accurate information, the numbers depicted on the website are indicative and may differ from the actual numbers in the main report. At Expert Market Research, we aim to bring you the latest insights and trends in the market. Using our analyses and forecasts, stakeholders can understand the market dynamics, navigate challenges, and capitalize on opportunities to make data-driven strategic decisions.*
Get in touch with us for a customized solution tailored to your unique requirements and save upto 35%!
The key factors propelling the market growth are the increasing awareness about CHI and robust pipeline activity globally.
Based on the diagnosis, the market is categorised into prenatal testing consisting of blood tests which include genetic tests and plasma sugar, among others.
Based on the treatment, the market is segmented into drug therapies and surgery, among others.
The treatment channels in this market are public and private.
The different regions in the acute coronary syndrome treatment market are North America, Europe, Asia Pacific, Latin America, the Middle East and Africa.
CAH is a series of autosomal recessive illnesses characterised by a deficit of an enzyme involved in the manufacture of cortisol, aldosterone, or both. The most frequent form of CAH, accounting for more than 90% of cases, is 21-hydroxylase deficiency caused by CYP21A mutations or deletions.
The key companies involved in this market are Eli Lilly, Novo Nordisk, Novartis AG, Rezolute, Inc., Eiger BioPharmaceuticals., Zealand Pharma A/S, Hanmi Pharmaceutical Co., Ltd., Crinetics Pharmaceuticals, Inc., and AmideBio LL, among others.
Explore our key highlights of the report and gain a concise overview of key findings, trends, and actionable insights that will empower your strategic decisions.
| REPORT FEATURES | DETAILS |
| Base Year | 2025 |
| Historical Period | 2019-2025 |
| Forecast Period | 2026-2035 |
| Scope of the Report |
Historical and Forecast Trends, Industry Drivers and Constraints, Historical and Forecast Market Analysis by Segment:
|
| Breakup by Diagnosis Method |
|
| Breakup by Treatment Method |
|
| Breakup by Treatment Channel |
|
| Breakup by Region |
|
| Market Dynamics |
|
| Supplier Landscape |
|
| Companies Covered |
|
Datasheet
One User
USD 3,299
USD 2,969
tax inclusive*
Single User License
One User
USD 5,499
USD 4,949
tax inclusive*
Five User License
Five User
USD 6,999
USD 5,949
tax inclusive*
Corporate License
Unlimited Users
USD 8,199
USD 6,969
tax inclusive*
*Please note that the prices mentioned below are starting prices for each bundle type. Kindly contact our team for further details.*
Flash Bundle
Small Business Bundle
Growth Bundle
Enterprise Bundle
*Please note that the prices mentioned below are starting prices for each bundle type. Kindly contact our team for further details.*
Flash Bundle
Number of Reports: 3
20%
tax inclusive*
Small Business Bundle
Number of Reports: 5
25%
tax inclusive*
Growth Bundle
Number of Reports: 8
30%
tax inclusive*
Enterprise Bundle
Number of Reports: 10
35%
tax inclusive*
How To Order

Select License Type
Choose the right license for your needs and access rights.

Click on ‘Buy Now’
Add the report to your cart with one click and proceed to register.

Select Mode of Payment
Choose a payment option for a secure checkout. You will be redirected accordingly.
Gain insights to stay ahead and seize opportunities.
Get insights & trends for a competitive edge.

Track prices with detailed trend reports.

Analyse trade data for supply chain insights.

Leverage cost reports for smart savings
Enhance supply chain with partnerships.

Connect For More Information
Our expert team of analysts will offer full support and resolve any queries regarding the report, before and after the purchase.
Our expert team of analysts will offer full support and resolve any queries regarding the report, before and after the purchase.
We employ meticulous research methods, blending advanced analytics and expert insights to deliver accurate, actionable industry intelligence, staying ahead of competitors.
Our skilled analysts offer unparalleled competitive advantage with detailed insights on current and emerging markets, ensuring your strategic edge.
We offer an in-depth yet simplified presentation of industry insights and analysis to meet your specific requirements effectively.

Share